Social Media Insights from MayoInOz
I attended the MayoinOz conference some time back and captured some of the key elements of the presentations and discussions
The core principle – Teamwork
http://â//platform.twitter.com/widgets.jsâ
If the #Mayo Bros had Twitter: “The best interest of the #patient is the only interest to be considered” #MayoInOz pic.twitter.com/lnxBOB17fC
— ANZCA (@ANZCA) November 14, 2016
We are being disrupted – captured perfectly in this one slide from Andrew Grills highlighting volumes of activity of WhatsApp vs the SMS text volume
Just in case you thought we had not moved to Digital: WhatsApp volume far higher than SMS text messaging #mayoinoz pic.twitter.com/Zdl4g6frw5
— Nick van Terheyden (@drnic1) November 14, 2016
http://â//platform.twitter.com/widgets.jsâ
Social is not a channel – although as several commentators pointed out many companies have jumped on the Social Media Band wagon and use it as another channel to pump content to potential customers
Top skills in demands as surveyed by LinkedIn feature data analysis and statistical
Moving to the cognitive era – Humans + Machines. It is not Artificial Intelligence but rather augmented intelligence
Test out your profile ith a Watson Analysis
http://gwen-systemu.mybluemix.net/
If the #Mayo Bros had Twitter: “The best interest of the #patient is the only interest to be considered” #MayoInOz pic.twitter.com/lnxBOB17fC
— ANZCA (@ANZCA) November 14, 2016
http://â//platform.twitter.com/widgets.jsâ
The last best experience has anyone has anywhere becomes the minimum expectation for the experience they want everywhere
This captures everything about competition
Your competitors are everyone – FedEx, Airlines, Hotels etc
So true. Think airlines/hotel rooms #MayoInOz pic.twitter.com/r7TXNRWP2L
— Michelle Carnovale (@M_Carnovale) November 14, 2016
http://â//platform.twitter.com/widgets.jsâ
Social Media Insights from MayoInOz was originally published on DrNic1
The Appliance of Science
Hurry up and Implement
Innovation has had a tendency to move at glacial pace and history is littered with scientific discoveries that took a long time to reach our world and have an impact on our lives.
Philosophiæ Naturalis Principia Mathematica – Wikipedia (Photo Wikipedia)
So many areas in our lives – math and complex numbers discovered in the 16th Century that were originally described as “imaginary” numbers as if to emphasize their impracticality and it was hundreds of years before they were used in earnest in calculations with alternating current and impedance. In physics, we have seen incredible insights from the basic observational details of Newton in the Philosophiæ Naturalis Principia Mathematica to Einstein’s astounding revelations in the Theory of Special Relativity and the Theory of General Relativity. The insights from these continue to provide breakthroughs in our understanding of the world
In Biology, Darwin’s theories contained in his book On the Origin of Species were deemed heretical at the time and yet now are considered to be the foundation of evolutionary biology.
Medicine proves to be no different and we have seen repeated instances of rejection and challenge to new technologies and insights. When René Laennec came up with the original stethoscope it was famously referred to in the Times of London:
“it will never come into general use notwithstanding its value. It is extremely doubtful because its beneficial application requires much time and gives a good bit of trouble to both the patient and the practitioner; and because its hue and character are foreign and opposed to all our habits and associations. It is just not going to get used.”
New Treatments Applied Slowly
It takes on average 17 years for an innovation to reach general application in healthcare – in this paper in the Journal of the Royal Society of Medicine 17 Years is the time for Translational Research. The authors reviewed multiple papers to ascertain the time delay in the application of medical insights into clinical practice. This table from “2000 Year Book of Medical Informatics Balas Boren Managing Clinical Knowledge for HC Improvement”
| Clinical Procedure | Landmark Trial | Current Rate Use (2000) |
| Flu Vaccination | 1968 | 55% |
| Thrombolytic therapy | 1971 | 20% |
| Pneumococcal vaccination | 1977 | 35.6% |
| Diabetic eye exam | 1981 | 38.4% |
| Beta blockers after MI | 1982 | 61.9% |
| Mammography | 1982 | 70.4% |
| Cholesterol screening | 1984 | 65% |
| Fecal occult blood test | 1986 | 17% |
| Diabetic foot care | 1983 | 20% |
To be clear I am not advocating the application of unproven ideas and theories but rather taking advances that have been proven with studies and expanding access to everyone.
Patient Engagement
We have seen multiple instances of patients who have refused to accept the current state of affairs in their conditions and treatment – Dave deBronkart (aka ePatient Dave) was an early advocate and trailblazer. In January 2007 he received a diagnosis of Stage 4, Grade 4 Renal Carcinoma and his prognosis was not good (that’s an understatement). Had he accepted the prognosis and the standard treatment he would not be here today. He did not and together with his care team he pushed the boundaries of the disease and our understanding and joined a clinical trial for a new therapy that was successful. 10 years on he is thankfully here and continues to advocate and push the boundaries of patient engagement and participation.
Not all therapies apply and not all patients are good candidates for new therapies but it’s a fair assessment that most of us would want a similar life-saving therapy for a catastrophic disease. Teasing out what works and what does not remains an ongoing challenge in science. Science and Discovery are littered with many blind alleys, failures and course corrections but it is these failures that contribute to our continued progress.

The new age of “all the data” is going to change the way we innovate and discover as Chris Anderson from Wired asked, “What can Science Learn from Google as he suggested, The end of Theory: The Data Deluge makes the Scientific Method Obsolete“.
At the petabyte scale, information is not a matter of simple three- and four-dimensional taxonomy and order but of dimensionally agnostic statistics. It calls for an entirely different approach, one that requires us to lose the tether of data as something that can be visualized in its totality. It forces us to view data mathematically first and establish a context for it later
Learning to use a “computer” of this scale may be challenging. But the opportunity is great: The new availability of huge amounts of data, along with the statistical tools to crunch these numbers, offers a whole new way of understanding the world. Correlation supersedes causation, and science can advance even without coherent models, unified theories, or really any mechanistic explanation at all.
Applying Knowledge Today
So now we are facing a future where information and discoveries are arriving at an increasing rate – look no further than the Exponential Medicine site (Part of Singularity University) and attend the great Exponential Medicine Conference that takes place each year in San Diego to get an idea of the Tsunami of innovation coming our way. So how do we capitalize on this increase knowledge acquisition so that the best information is applied each and every time we look for insights and treatments in medicine.
Incremental Improvements to Adoption of Innovation
For the incremental approach, it’s turning these insights into small actionable pieces that can be applied at each of the intersection points
- It’s making the information available in its entirety to everyone involved in the care – this includes not just the clinicians but also the patients and their family and friends (with the approval of the owner of the data – the patient)
- Abolish Selective reporting – Make the research data widely available and importantly publish all the data, not just the data that matches the desired outcome or result
- Be open to change and alternatives – recognize the resistance to change is inherent in all of, acceptance can be the first step in change
- Find common ground and practice guidelines where possible to reach agreement and limit the variation in care that occurs in treatment that comes with your location and treating entity
Do you have any better suggestions? What small change have you seen that makes a difference to speed up the appliance of science in healthcare? What one thing could we do that would have a big impact in this area?
You can also follow me here on medium, on twitter, or on facebook
Why The Patient Story Should Always Take Center Stage
I recently discovered that one of the great storytellers of our day – Malcolm Gladwell has a new podcast – Revisionist History. Each episode (he is now into Season 2) takes a look at some piece of history and through some delightful storytelling revisits the history and our perceptions of events. It reminded me of this piece I wrote some time back focused on the importance of storytelling in and the history we capture from our patients.
The Patient Story
Stories are the backbone of who we are. They provide context, insight, subtle and not-so-subtle hints about ourselves and those around us. They teach us lessons and help us determine similarities and differences so that we can avoid mistakes and replicate success.
Much like Malcolm Gladwell’s new podcast, the popular Serial podcast is dedicated to deeply exploring different narratives, stories, and evidence, in order to find insight into a mystery. I found it fascinating for myriad reasons, but mostly for the way it was told. And, at the beginning of each episode is the reminder: “This is Serial: one story told week by week.”
It’s engaging and thought-provoking, but what I like most is that it forces the listener to consider the same principle case from different perspectives. I was struck by how similar this journalistic process of poring over reports and talking with people to hear their perspectives is to the art of medicine. When a patient comes to see you with a set of symptoms, you have your checklist: you examine him, you ask questions, maybe order lab tests.
If your patient’s condition persists, you might talk to his son, who brought him into the follow-up appointment, and he might mention something his father had forgotten or dismissed as irrelevant. You carefully listen to what is said, and what is not said, noting anything that is out of the ordinary. You use that patient’s chart as your journalist’s notepad.
The Luxury of Time
The difference is that physicians don’t always have the luxury of time. Whether it’s because treatment decisions need to be made or there is a line of patients waiting to be seen, they need to have quick access to the most relevant data and best practices so they can make informed decisions and recommendations to their patients. They need to be able to collaborate with a specialist to look at a medical image and report together, discussing whether that secondary finding is something more than it appears.
Compounding matters are that as the healthcare industry awkwardly shifts to value-based care, physicians have been forced to precariously straddle the line between two oppositional models, and amidst it all, they try desperately to not let the tumult affect their patients. They’re beholden to the regulatory bodies that govern how they practice and they have sworn an oath to protect and care for those who have entrusted them with one of their most valuable gifts: their health.
As Drs. Patrick Ober and William Applegate so eloquently as succinctly articulated in their recent article “The electronic health record: Are we the tools of our tools?”:
“Attentiveness to the nuances of communication is an essential attribute of a skilled physician; in its quest for medical standardization, the EHR discourages nuances and promotes functional medical illiteracy.”
Time Pressure is Killing the Story
Physicians are being forced to make hard choices, and one of these sacrifices often comes at the expense of the patient story. And when you lose that story, the patient becomes a collection of somewhat unconnected data points. This has a profound downstream impact as the next attending physician will have to go through the same rigorous exercise of asking questions and sleuthing around, which not only frustrates the patient, it can lead to unnecessary wasted time.
The overall health IT endgame is the right one: creating a continuous and integrated care cycle that helps drive the best care outcomes. While technology is a key component in the healthcare ecosystem, it should only play a supporting role. It helps sifts through the massive amounts of data and appeases the regulatory requirements so that the physician can listen attentively to his patient as she walks him through the series of changes and symptoms she has experienced.
In healthcare, the story is everything. Nothing happens in a vacuum. As physicians, it is our responsibility to listen to our patients and their family members, noting the details, and helping them understand and treat their symptoms. We can’t do this if we’re not paying attention.
Capturing the Story
It’s not a lack of willingness on the part of the healthcare professionals but rather the time pressures of other tasks that have precluded the capture of the story. What small improvements could we make in the system to increase the time for patients to share their story?
- Maximizing the time with the clinician requires we ease the burden of administrative tasks from the clinical team
- Identify any tasks that can be carried out by others – simple administrative functions that could be assigned to other members of the team
- Patient engagement can occur long before the face to face visit with their clinicians and allow patients access to their records and the ability to validate and update their information
- Move the healthcare payment model to value-based care and drop the requirement of documentation for the purposes of billing would change the focus of the consultation to be clinical, not financial
This is an important area for clinicians – we recognize the value of the history and to this day the history still contributes some 80% to the diagnosis of a patient’s condition. This alone should provide the impetus to change the system to allow the patient story to be front and center.
Do you have any better suggestions? What small change have you seen that makes a difference in the use of Telehealth services. What one thing could we do that would have a big impact in this area?
This piece originally appeared on HITConusltant
You can also follow me here on medium, on twitter, or on facebook
Employee Empowerment to Help Patients
Delivering Outstanding Service

I had a frustrating experience with a bank this week that had so many opportunities for correction and improvement. The short version was a requirement to follow a policy that no one could explain requiring additional steps necessary because the bank had taken so long to follow their process. At various points, the employees were forced to follow a senseless protocol and policy and given no flexibility. In some cases, it may not be possible to bend policy – perhaps because of regulatory requirements but when we reached of an extraordinarily frustrating experience I tried to tease out an apology or even an acceptance that perhaps this was not the best outcome and there might have been a better way. The lack of employee empowerment prevented them from accepting any responsibility, offering an apology and they were firmly stuck to a script filled with hollow “I understand your frustration” statements.
Healthcare and Satisfaction
There is an interesting connection between the soft aspects of the patient experience and customer satisfaction. The actual clinical experience and quality is important – and some would suggest the most important component. But in talking to patients, simple aspects of the experience that included reducing waiting times, personal interactions and communications. But if the staff are not enabled to deliver a good experience and find themselves pressured by production metrics that preclude the important human connection and support that patient crave. It is easy to lose sight of the human elements as we strive for efficiency and the system pushes us to squeeze more and more cost out of any activity.
Customer is Always Right
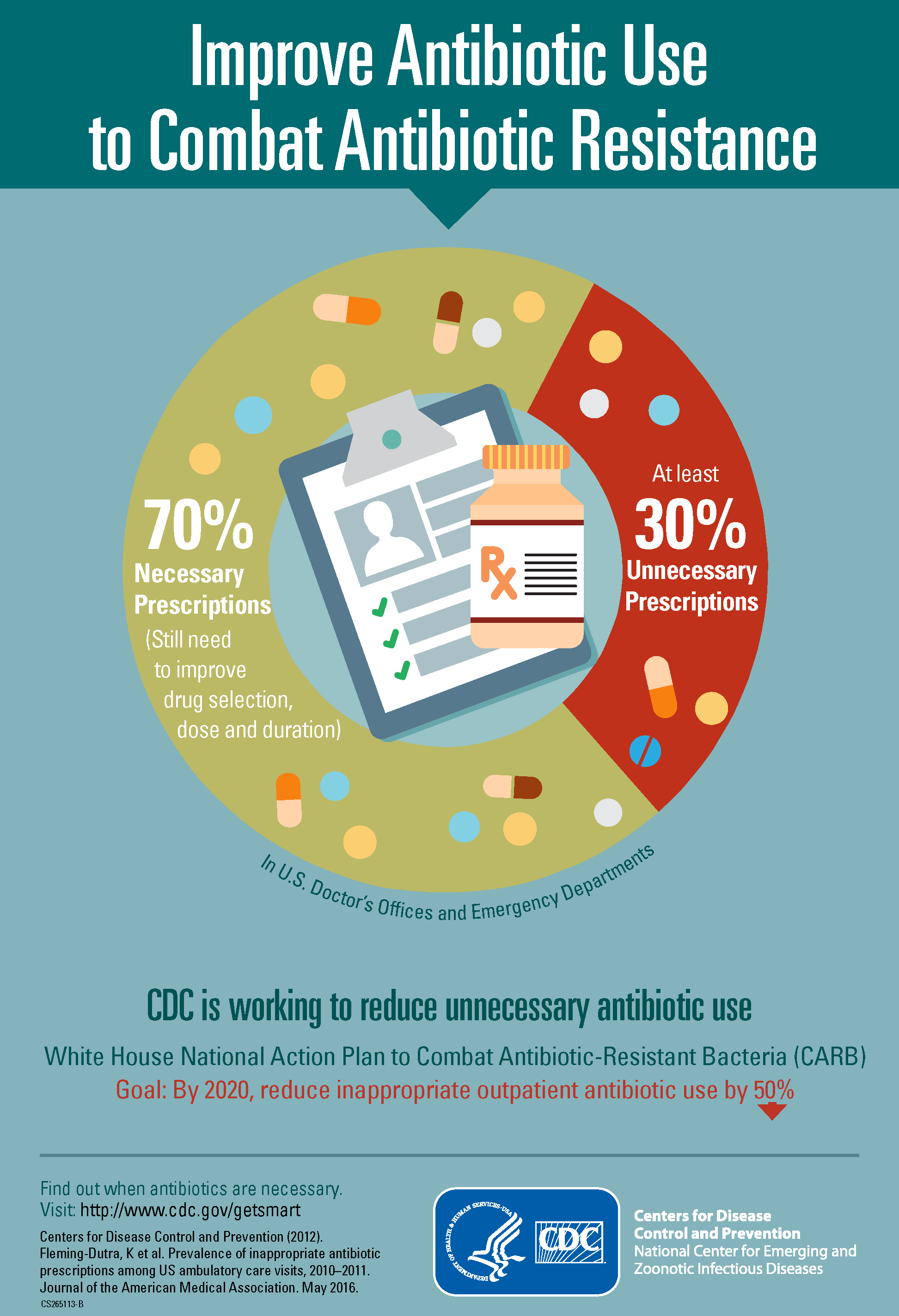
This is an age-old adage that no matter what “The Customer is always Right”. In healthcare, this can be a difficult strategy especially when given the poor information available for making decisions and the inherent bias built into our system to provide unnecessary care. Take the prescribing of antibiotics that has reached epic proportions that recent data suggests has reached levels as high as 30% that are unnecessary.
Incremental Improvements in Employee Empowerment
Recognizing the challenge of changing policy which can be a long journey my suggestions for incremental improvements start with empowerment
For any staff that deal with patients/customers
- Empower your employees to make localized instant decisions
- Provide them with a set fo guidelines on what they can do and offer
- Set the boundary conditions but empower them to respond in cases of unhappy/upset patients
- It could be as simple as offering a Gift Card for a Coffee or Snack accompanied by a genuine heartfelt apology
- Provide a pathway for problems to be reported, reviewed by the team with input from everyone and accept suggestions and ideas on how things could have been improved or even fixed
You won’t just get happier patients – you will get happier employees
Do you have any better suggestions? What small change have you seen that makes a difference empowering your employees? What one thing could we do that would have a big impact in this area?
You can also follow me here on medium, on twitter, or on facebook
The Internet of Things Changes Everything in Healthcare

The Internet of Things is Changing Everything in Healthcare
While there remains some resistance to the idea of tracking everything there is increasing use and now results from the IoT. It ranges from the simple – weighing scales that record and report weight loss and gain, not just for health and fitness but as an early indicator of problems in Congestive Heart Failure to the complex ideas of tracking pills and compliance with RFI tagged medication
Expect this sector to explode
The Internet of Things Changes Everything in Healthcare was originally published on Dr Nick – The Incrementalist
Telehealth for Everyone
Working from Home

Americans are doing more and more activities from the comfort of their home and its no surprise – the frustration of showing up to a business only to find they are closed or worse short staffed and instead of dealing with the customer in front of them the staff are on the phone answering queries. Bypass the line and move to the front of a virtual queue from the comfort of your own home is appealing.
Online Queuing Systems
There is even sophisticated queuing mechanism when there is limited availability for a resource as I discovered when I tried to score tickets to the Harry Potter show in London
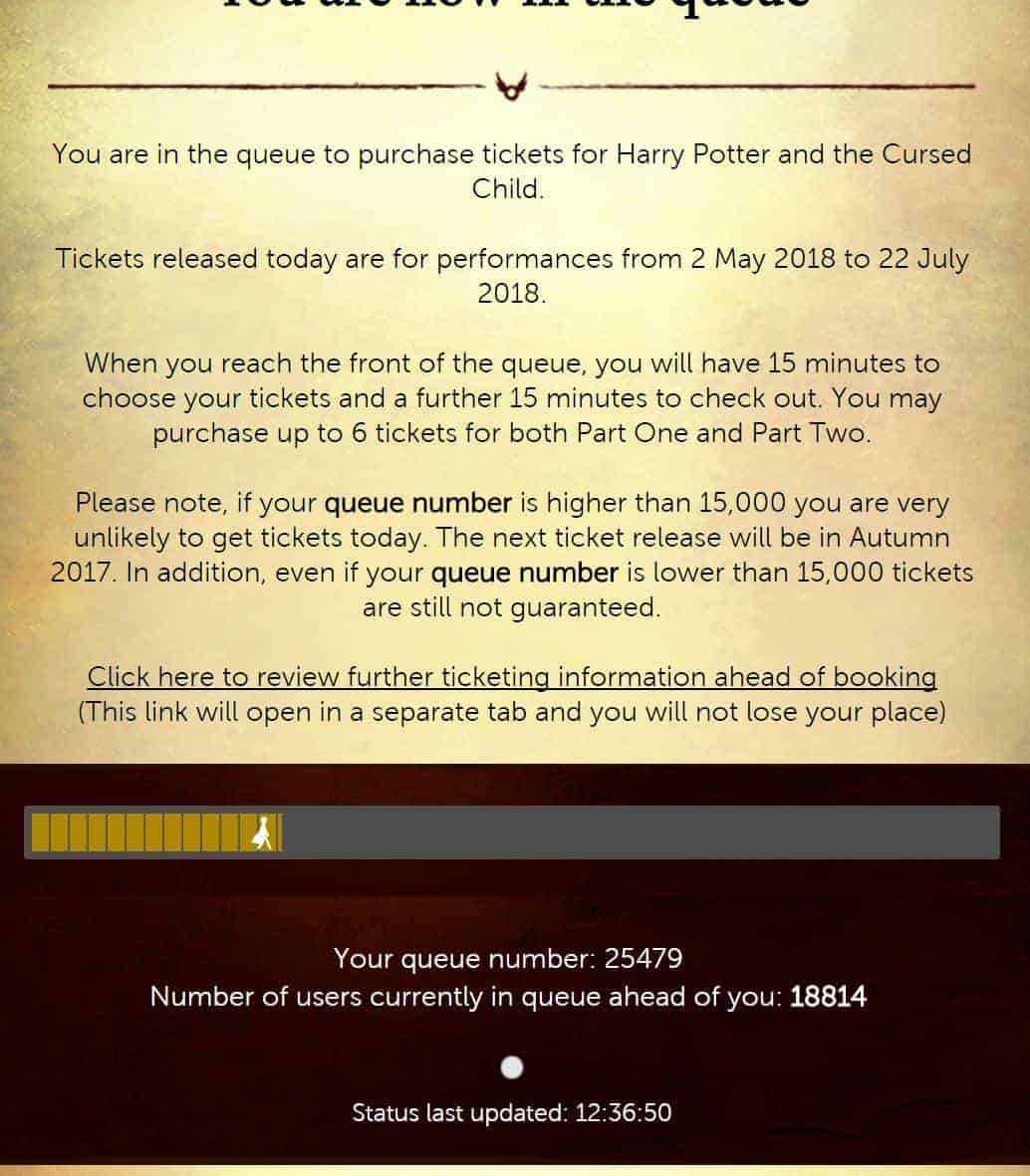
You had to be quick to join this queue virtually
This experience was managed comfortably from my laptop as I sat sipping coffee and checking in occasionally while I continued to work on other things on my laptop. I think it would have been an even bigger disappointment to have spent that time in a line somewhere only to find there were no more tickets left by the time it was my turn.
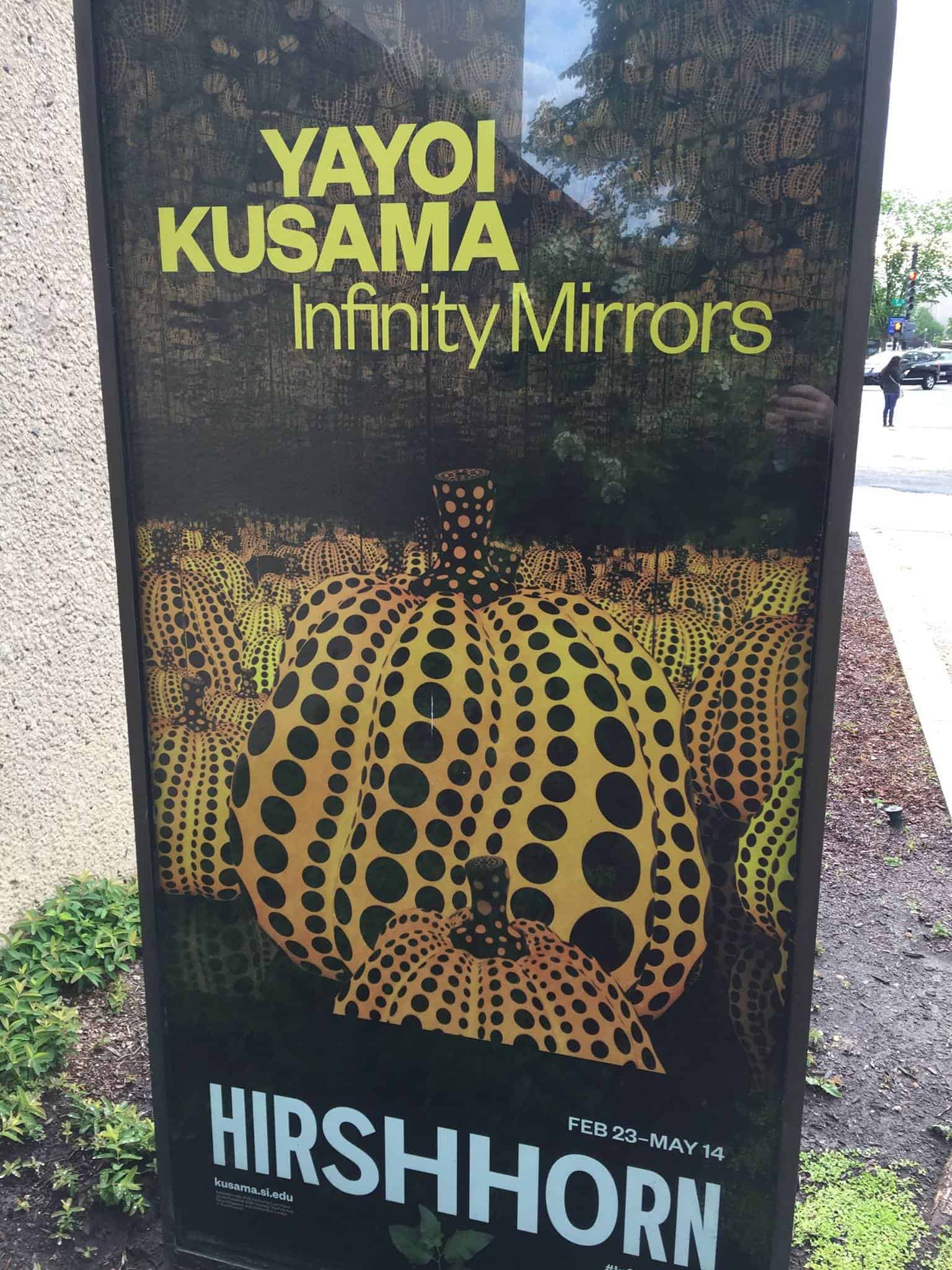
Compared to my experience getting tickets to the Kusama Infinity Mirrors Exhibition at the Hirshhorn Museum which was a physical process I went through recently having failed to score tickets in the online system. This process required early rising, driving into town, expensive parking and then standing in line for 4 hours to get a ticket (it was worth it)
Getting an Appointment
Telehealth has many of the same elements to recommend it. The hassle of making an appointment – which in a recent post online was filled with frustration that started with doctors offices, not taking new patients and the ones that did not have available appointments for 6 months! Assuming you can make it past this assault course and get an appointment that is convenient for you the system requires driving to the office, sitting in a waiting room and being subjected to loud obnoxious daytime television broadcast while you wait for your physician encounter that could last minutes. Some physician exams do involve more serious health issues, but most are routine visits to refill prescriptions and see to minor illnesses and infections, needs that could easily be met with video chat.
Why Has Telehealth Not Taken Off
Discussing this with a colleague recently he highlighted the fact that the leaders of the American Telemedicine Association were famous for saying “This is the year for Telehealth”, every year for the past 20 years
This reminds me of an article I wrote back in 2005, I wrote a piece that continues to show up in my inbox as being used and linked to. It was featured in the Health Management Technology Journal titled “Is Speech Recognition the Holy Grail”. I was frequently quoted and referenced as saying
“Speech Recognition has been 2 years away for the last 10 years and its still 2 years away”
So what happened and why do studies suggest that instead of reducing visits and costs it has the opposite effect? Telehealth drives up healthcare utilization and spending – yes you read that correctly. The report, published Monday in the journal Health Affairs, found that although telehealth appointments are cheaper than in-person and emergency room visits, the online and virtual resources encourage vast new utilization, ultimately driving up healthcare spending
The report, published Monday in the journal Health Affairs, found that although telehealth appointments are cheaper than in-person and emergency room visits, the online and virtual resources encourage vast new utilization, ultimately driving up healthcare spending
In one of those perverse unintended consequences – providing easy(ier) access to healthcare services
The convenience of telemedicine is encouraging people to seek care when they normally wouldn’t, ….You don’t even have to go anywhere … you just have to pick up the phone
Their recommendation – encourage more cost sharing for consultations to encourage patients to think more critically what they elect to seek a medical consultation for. It’s a familiar argument and one that circulated frequently amongst General Practitioners in the United Kingdom’s National Health Service (NHS) who faced a barrage of requests for care at all hours of the day, night and weekend for conditions that were either trivial or at a minimum non-urgent. But when a service is valued at zero (that’s not to say that it has no value just that the perception is that it has a value or cost of zero) the usual filters fail to be applied.
Healthcare is Different
Normal economic models are hard to apply in healthcare – introducing a co-pay or shared cost model has its own set of unintended consequences. Too high and you discourage legitimate requests for help from patients and this typically affects the vulnerable and poor disproportionately. Too low and it fails to influence the behavior sufficiently to warrant the additional administrative burden and overhead of introducing these mechanisms. But that is true too in other industries – we pay for our own car maintenance and don’t look to the car insurance provider to pay for tire and brake replacement. But when funds are tight people will avoid maintenance and check-ups that ultimately could have saved significant damage and higher costs of repair. But failure in healthcare can be catastrophic and life ending – a car is just a car.

Ultimately I think it requires a retraining of the individual in better self-care and management and a stronger closer relationship with a trusted healthcare professional who is seen as a partner in the process. I have that with my local garage – I found through a personal recommendation and am a loyal user for years. I have a trusting relationship – unlike some of my experiences with garages that have set up programs that incentivize the employees to sell unnecessary services and repairs this garage does not. The inflection point for me in trust was the time I took one of my cars in to solve an intermittent problem – they had the car for 2 days trying to replicate and diagnose and ultimately were unable to reproduce the problem and could find no underlying problem – the charge for the service – zero. When I asked why I was told they had carried out no maintenance or repairs.
![]()
We can achieve the same in healthcare but it requires centering the services around the Primary Care and the Medical Home. I made this point in this piece Give consumers the telehealth option they really want: Virtual visits with their own doctor. Separating out services is like going to the cheap oil change shop like Jiffy Lube. You can get a cheaper oil change and check up but their model is designed to identify problems and sell you on other services. In some cases, I’ve had recommendations for additional services only to be told by my trusted mechanic they are not required.
The Telehealth service providers offer a valuable and important tool – even more so for some rural communities and places that have limited access or low penetration of available clinical professionals – but ultimately if the care is not integrated it will likely have the tendency to increase utilization and has the effect that my colleague described of increasing visits to your healthcare providers.
A telehealth doctor or nurse practitioner can give great episodic care, but those episodes don’t look at the whole patient. Patients also need someone who looks at their risks for chronic disease, such as obesity, type II diabetes and high blood pressure, and guides them toward lifestyle choices that prevent those diseases. And patients also need someone who can connect the dots — a provider who knows and understands their history and can view current symptoms in the context of the patient’s overall health. That’s tough to do if you see a different provider every time, especially if that provider does not have access to your records when he or she writes a prescription or suggests a treatment. It’s why emergency rooms are not a good place to get primary care — not only is it expensive, but the doctors often lack access to critical information.
Integrated Telehealth
To avoid telehealth becoming a cheaper version of emergency room care we must connect telehealth to patient-centered medical homes and offer our clinicians a means to offer this service as part of their total package. We see the early stages of this albeit for an elite few that can afford it with Concierge Practices (The Doctor Is In. Co-Pay? $40,000) that customize care. Reminds me a lot of the service the General Practitioners have offered and still do in England as part of the NHS with home visits included. But enabling this for more people will require some changes to the system especially the reimbursement model that currently incentivizes activity, not wellness or care. Providing technology to offer support and guidance around minor ailments and triage the limited clinical resources directing patients to access them when necessary would help. The Family Practioner with the patient becomes the conductor and manager supporting the delivery of care and drawing on the necessary resources. Their capability is extended through Telehealth allowing them to interact with many more patients remotely and saving unnecessary trips to the office but being rewarded for the care management.
Incremental Improvements in Telehealth
We have been on the cusp of acceptance and widespread roll out for a long time – finding some small step towards that in your practice or as a patient would help move more people to this model and begin showing the value. From the patient consumer perspective being open to the channel and using it where available in lieu of care to understand the experience would help. Think back to when airlines first offered kiosk check-in. Were you one of the many people who said not me ever….. and now it’s your preferred method?
- Accepting the value of remote access and using the existing technology in place can help jump start the process
- Telehealth can be as simple as a telephone call – for some of the major providers that are a big part of the service they offer
- Adding simple video chat will help expand the channel and allow an exploration of the medium to understand better how it can apply – perhaps starting unofficially with family
- Make Telehealth one of the channels that your Patients can Access you – the reimbursement models may not support this model quite yet but it will undoubtedly induce loyalty and improve the care
Do you have any better suggestions? What small change have you seen that makes a difference in the use of Telehealth services. What one thing could we do that would have a big impact in this area?
You can also follow me here on medium, on twitter, or on facebook
Treating Mental Health
Don’t judge my path if you haven’t walked my journey
Mental Labels
Just the term “Mental” induces reactions and responses from every corner of our society, and mostly they are not positive. Perhaps part of the problem can be attributed to the broad and different definitions applied to the term that includes its use as an adjective relating to the mind or disorders of the mind but it also has an informal us as “insane” or “crazy”
It’s no wonder that when we refer to someone as having “Mental problems” or a “Mental Condition” – so perhaps we need to change the terminology to start addressing “Mental” health as part of our overall health. The precision of language and terminology is important but we have a tendency that appears to be increasingly misused, or perhaps it just appears that was because it is magnified by social media and the 24/7/365 news cycle. For example, the term “Depression” is a clinical diagnosis that has some very specific symptoms and durations but the term is used excessively in place of sadness, misery, or sorrow. SO for this article, I will refer to “Diseases of the Brain” rather than “Mental Disorders”
Part of Physical Health
A recent article by John Campo, MD, Professor, and chair of the Department of Psychiatry at Ohio State University pointed out the mismatch between the prevalence and impact of diseases of the brain and the lack of legitimacy as a “real disease
The treatment of mental illness has long been held back by the sense that disorders of emotion, thinking, and behavior somehow lack legitimacy and instead reflect individual weakness or poor life choices
Some of this likely stems from our lack fo understanding relative to brain disorders evidenced in history by the way we viewed and “treated” anyone deemed to be unusual or different. These attitudes date back to at leat the 13th Century and “St. Mary of Bethlehem” in London built in 1247 and used as an institution for the insane. It was colloquially referred to as “Bedlam” hospital (yes that is where the term “Bedlam” came from) that featured horrific treatments from “rotational Therapy”

Imagine being stuck on the Mad Hatters Tea Cup ride at high speed for hours
And extended to beatings, bloodletting, and starvation! This sordid history is covered by the Museum of Healthcare Blog. This attitude extended into my medical school training where we were dispatched to Friern Hospital (formerly Colney Hatch Lunatic Asylum) that at its peak was home to some 2,500 patients with disorders of the brain. My clinical experience there included a harrowing personal experience that still shapes my behavior to this day.

Long corridors with Wards radiating out
Moving to Whole Care
The disconnect between the specialty of Psychiatry and the rest of medicine is rooted in our inability to observe and explain the workings of the brain. Even some of our treatments work but we struggle to understand why or how. This manifests in the challenge of honest acceptance of having a disease of the brain and being able to find help to treat that condition. For most people, our exposure to this world is limited to the Hollywood lens, like “Awakenings” starring Robin Williams and Robert de Niro
It is sad to note that Robin Williams suffered a sometimes public struggle with a brain disorder and ultimately committed suicide secondary to his suffering of Lewy Body Dementia
Based on the true story and book “Awakenings” written by Oliver Sachs – the British Neurologist, naturalist, and author who died back in 2015. He was a prolific writer who wrote with such eloquence and mastery of language you can lose yourself in his books.
‘Healing’,
Papa would tell me,
‘is not a science,
but the intuitive art
of wooing Nature.’
The Art of Healing – W.H. Auden
Science is Helping
The good news is that technology and science are helping as we unlock some of the mysteries of the brain’s function and the diseases that impact function. In fact, in many instances, we are discovering that the brain plays a much larger role in many diseases and we ignore this at our peril. We continue to unlock the chemical and physiological functions in the brain and as the science advances so too does the integration of the specialty psychiatry under the same roof as the rest of medicine.
There are now a number of initiatives working to expand our understanding, coordinate research, results, and findings that included the 2013 announcement by President Obama for the “BRAIN Initiative” (Brain Research through Advancing Innovative Neurotechnologies) that is homed at the National Institute of Health (NIH) and complemented by the The Human Brain Project from the European Union. The initiatives are not without problems and uncertainty of funding continues to challenge progress but understanding, science, and data remain a central requirement to progress.
There are some areas of progress from industry and Arshya Vahabzadeh, MD, the Chief Medical Officer at Brainpower has been championing Virtual Reality and Augmented Reality as a tool to help the growing population of Autism patients handle the complex world of emotions and human interactions. As he highlighted Virtual and Augmented Reality was a hot topic at the recent American Psychiatric Association Meeting
A post shared by ᎪᎡᏚᎻYᎪ ᏙᎪᎻᎪᏴᏃᎪᎠᎬᎻ Ꮇ.Ꭰ. (@psychsuperman) on May 31, 2017 at 9:18am PDT
And was featured in this Medscape article: Virtual Reality a Game Changer for Psychiatry (Medscape)
Incremental Improvements in Brain Disorders
As Dr. Campo pointed out
Better understanding of the human brain and the biological nature of the mind will help, but it won’t be enough. How we think about mental health matters. When mental health is ultimately recognized as essential to physical health, not an extraneous element of it, then we will have access to true, complete, modern medicine
Changing the narrative and words may seem trivial but for any change to take place we need education and awareness that removes the stigma and fear associated with disorders of the brain and deliver the same compassion and care that patients with cancer or heart disease receive.
So my thoughts for some incremental improvements you can make addressing disorders of the brain
- Words Matter – it’s not “Mental Health/Disorder” – it is Disease or Disorder of the Brain
- Ask, listen and most importantly digest and be there as we interact with others – read Maneesh Juneja blog – Being Human
- From a clinical perspective – the clinical history and the detail of the Presenting Complaint and History of Present Illness remain the mainstay of diagnosis and understanding
- Read or listen to Oliver Sach’s – you can find his books – or watch his TED Talk, or hear him on Science Friday or NPR or read one of his articles
What small change have you seen that makes a difference in the support of people with disorders of the brain. What one thing could we do that would have a big impact in this area?
You can also follow me here on medium, on twitter, or on facebook

leave a comment